Search the Library
NOTE: This is a new search platform (as of May 2026). If you do a search and don’t get the results you were expecting, please email us at ctnlib@uw.edu to let us know? (If possible, please share your exact search strategy. Thank you!)
Enter keywords and hit Enter (or click the magnifying glass) to search. You can then also select document type or subject/topic to narrow results further (or just use those for searching without a keyword). Results display below this search form.
Document types
Subjects
- CTN-#### format for protocols (CTN-0001, e.g.)
- “exact phrase” (if phrase is not found, it will return results that contain all terms
- word1 NOT word2
- word1 word2 (finds both words)
- Click title to access full-text
- “Show details” reveals abstract & other info
- Checkboxes select items for copy/pasting or printing
- Need help getting a copy of a journal article?
Email ctnlib@uw.edu
Search results

Background: While medication for opioid use disorder (MOUD) is effective for a significant proportion of patients, many return to using opioids during treatment. Understanding which factors lead to successful treatment informs the development of implementation approaches that can improve outcomes. This manuscript and its accompanying website provide an applied introduction to interpretable machine learning for clinical investigators interested in predicting treatment response for people using MOUD.
Methods: This study, which uses data from CTN-0094, applied machine learning (ML) algorithms (K-Nearest Neighbors (KNN), logistic regression with and without regularization, Multivariate Additive Regression Splines (MARS), Support Vector Machines, Classification and Regression Trees (CART), Random Forest, Bayesian Additive Regression Trees (BART), Boosted Trees, Neural Networks) to predict failure of treatment in a collection of 2478 individuals who had participated in the three largest pragmatic, clinical trials of MOUD.
Results: All models produced Receiver Operating Characteristic Area Under the Curve (ROC AUC) estimates in the range of 0.62 to 0.67 using cross-validation data and the optimal model, random forest, achieved 0.65 using testing data. The algorithms nearly universally identified predictive features such as age, intravenous drug use days, study medication, and study site. Most algorithms also identified various aspects of smoking. Only the algorithms that detect complex non-linear trends identified details from timeline follow-back. One algorithm, BART, performed well while devaluing all treatment-specific details.
Conclusions: After explaining how to apply, compare, and contrast various ML workflows, the results show that while overall modeling performance is similar across the models developed, the use of different algorithms identifies different sets of predictive features. Previous research has not recognized some features as important for predicting treatment outcomes. A companion website introduces clinical investigators to the concepts and implementations this study presents. That site also provides a detailed annotated blueprint to fully replicate, or even expand, this work.
Related protocols: CTN-0094
Cocaine use disorder (CUD) is a major public health issue, and greater cocaine use severity has been associated with worse treatment retention and outcomes. Therefore, greater understanding of processes that influence cocaine use is needed. Both anhedonia (i.e., undervaluation of nondrug rewards) and cocaine demand (i.e., cocaine valuation) are related to cocaine use severity and thematically related to each other at face value, but no studies have directly compared these outcomes to our knowledge.
The present study represents a secondary analysis from a two-phase sequential, multiple assignment, randomized trial aimed at developing adaptive interventions for CUD (CTN-0130). We examined the relationship between anhedonia and cocaine demand and how these measures were related to cocaine use severity. Participants (N = 116) were treatment-seeking adults with CUD. All measures were taken at baseline before treatment initiation. Analyses revealed (a) moderate and very strong evidence of relationships between cocaine demand factors (i.e., persistence, amplitude) and anhedonia (PP values ≥ 77.8%); (b) positive association between cocaine demand (both persistence and amplitude) and measures of cocaine use severity, with the exception of one relationship, which was in the opposite direction; and (c) demand amplitude continued to be positively related to cocaine use severity, even when considering anhedonia.
Conclusions: Overall, findings from this study indicate cocaine demand relates to cocaine use severity more strongly than anhedonia.
Related protocols: CTN-0130
This is the Primary Outcomes Article for CTN-0130.
Fentanyl-related, cocaine-overdose deaths have drastically increased, yet research on how people who use cocaine perceive fentanyl adulteration is limited. This study developed the novel Adulterated Cocaine Purchasing Task, a modification of the original Cocaine Purchasing Task, to quantify how people respond to fentanyl adulteration in cocaine.
In the Adulterated Cocaine Purchasing Task, participants indicated how much cocaine they would purchase when cocaine had no (0%) versus some (10%) probability of fentanyl adulteration. Study aims were to (a) determine how possible fentanyl adulteration affects cocaine demand and (b) determine which individual characteristics predict continued demand for cocaine despite fentanyl adulteration.
This Amazon Mechanical Turk study included self-reported cocaine purchasers (N = 64), who completed self-report questionnaires (demographics, substance use history, depression/posttraumatic stress disorder symptoms, fentanyl knowledge quiz), and the Adulterated Cocaine Purchasing Task.
Results showed (a) that a greater probability of fentanyl adulteration (10%) lowered cocaine demand, but only for intensity (Q₀; amount of cocaine consumed when free; p < .001); (b) no effect on other demand indices (Omax, Pmax, essential value, breakpoint); (c) significantly more zero responders with 10% probability of fentanyl adulteration than 0%, p < .001; and (d) that opioid co-use, depression, age, posttraumatic stress disorder, fentanyl knowledge, and cocaine use severity did not moderate the relationship between fentanyl adulteration and intensity.
Conclusions: Overall, fentanyl adulteration reduced cocaine demand but only for volume preferred at minimal cost, not general motivational drive for use, illustrating the dangerous insensitivity to toxic contamination. The internal validity of the paradigm provides proof-of-concept for this approach to identify individuals at risk from fentanyl-adulterated cocaine.
Related protocols: CTN-0130

This commentary piece describes how the clinical benefits of research extend far beyond testing the effectiveness of treatments. Drawing on findings from CTN-0099 (the ED-INNOVATION trial), the author highlights how participation in a clinical trial led to institutional practice changes, career development for clinicians, and stronger community engagement, with one participant reporting that participation in the trial “completely changed the culture of our ED.” Clinical research also has economic benefits, as investments in research funding support jobs and other local economic activity. Additionally, hospitals and clinicians involved in clinical trials often demonstrate better adherence to evidence-based practices and improved patient outcomes (the “trial effect”). Overall, the author argues that the benefits of clinical research extend beyond studies that demonstrate the efficacy of a new treatment or change in practices. Strengthening connections among researchers, health systems, clinicians, and communities can amplify the impact of clinical research and improve both patient and population health outcomes.
Related protocols: CTN-0099
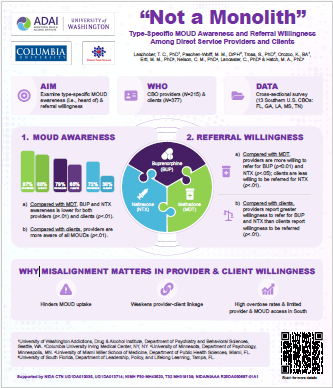
Poster describing a study that examined type-specific medications for opioid use disorder (MOUD) awareness (i.e., heard of) and referral willingness among CBO providers and clients. The data was acquired via cross-sectional survey of 13 Southern U.S. CBOs in FL, GA, LA, MS, and TN. Analysis revealed that compared with methadone, buprenorphine and naltrexone awareness is lower for both providers and clients, though providers are more aware of all types of MOUD than clients. Additionally, providers report greater willingness to refer for buprenorphine and naltrexone than clients report willingness to be referred (especially for naltrexone).
This type of misalignment can hinder MOUD uptake, weaken provider-client linkage, and contribute to high overdose rates and limited provider and MOUD access in the South.
Related protocols: CTN-0082
Introduction: Despite rising concern about overdoses from fentanyl-adulterated cocaine, research on responses to adulteration among people who use cocaine (PWUC) is limited. We aimed to identify what risk mitigation strategies PWUC would engage in if they suspected fentanyl in their cocaine. Secondarily, we tested whether key individual differences were related to use of risk mitigation strategies.
Methods: A secondary analysis of an online study (CTN Protocol ID: CTN-0130) collected responses from 97 self-reported cocaine purchasers. Participants completed questionnaires on demographics and substance use and reported what they would do if they found out their cocaine might contain fentanyl. Participants selected from a list of behaviors (with a free response option). Responses were coded into a four-level variable: “no change,” “transfer risk,” “harm reduction,” and “abstain.”
Results: About 16.5% endorsed no change in their behavior, 14.4% endorsed transfer risk, 25.8% endorsed harm reduction, and 43.3% endorsed abstain. Of the 10 individual differences tested only cocaine use frequency and previous personal experience of overdose significantly related to selected behaviors. Further analysis showed those with more frequent cocaine use, or prior overdose experience were more likely to use cocaine normally or transfer risk rather than use harm reduction or abstain.
Conclusion: While 83.5% of our sample reported they would attempt to mitigate risk if they suspected fentanyl in their cocaine, participants with more frequent cocaine use or a prior overdose endorsed less use of typical harm reduction or abstention. This highlights the need to direct harm reduction interventions to PWUC to mitigate the fentanyl overdose risks.
Related protocols: CTN-0130

Substance use can be a coping mechanism during stressful times. The United States opioid crisis worsened during the COVID-19 pandemic. This study looks at the effects of the pandemic on self-reported change in drug and alcohol use and medications for opioid use disorder (MOUD) and naloxone interest in a population and region hit hard by the opioid crisis—people who use illicit opioids (PWUO) and other drugs in the Southern United States. Cross-sectional data came from the National Institute on Drug Abuse Clinical Trials Network survey study CTN-0082. During the pandemic, participants (N=381) completed a survey about their pandemic-attributed increase, decrease, or no change in use of opioids, non-opioid drugs, or alcohol and interest in MOUD and naloxone. Data were analyzed using multinomial logistic regressions; regression models included potential contributing factors like sociodemographics, substance use frequency, and psychological distress. Results showed that most participants reported no change in: use of opioids (54%), non-opioid drugs (59%), or alcohol (64%) and interest in MOUD (60%) or naloxone (72%). Factors related to no change in relation to change in substance use and/or service interest included past 12-month substance use frequency, race, ethnicity, age, sex, and education.
Conclusions: We conclude that the lack of change in drug use and interest in MOUD and naloxone suggests stability amidst challenging times in our sample of PWUO in the Southern United States. Differences in outcomes based on sociodemographics and substance use frequency indicate the need for tailored services during future public health emergencies.
Related protocols: CTN-0082

Introduction: The initiation of buprenorphine for patients with opioid use disorder (OUD) in the emergency department (ED) has been associated with improved outcomes including reduced ED visits and increased treatment engagement. Though both standard-dose (8 mg buprenorphine equivalent) and high-dose (24 mg buprenorphine equivalent) strategies to initiate buprenorphine have been used in the ED, no prospective trials comparing outcomes among patients receiving these treatments have been reported.
Methods and analysis: This multisite randomised clinical trial (CTN-0145) is a multisite double-blind, double-dummy, randomised clinical trial enrolling 360 emergency department patients with moderate-to-severe OUD. Enrolled patients will be randomised to one of two study arms: standard-dose induction or high-dose induction, both provided in the ED. This study will engage, train and provide resources to five EDs throughout the US to recruit patients with untreated OUD into a randomised clinical trial. The primary aim is to evaluate the effects of the standard-dose induction and high-dose induction on rates of OUD treatment participation within 10 days post-randomisation. The secondary aims are to evaluate differences between standard-dose induction and high-dose induction on the outcomes of opioid craving, opioid withdrawal symptoms and illicit drug use assessed during 10 days post randomisation and evaluate the effects between treatment arms on rates of OUD treatment participation within 30 days post randomisation.
Ethics and dissemination: This study is funded by the National Institute on Drug Abuse and has been approved by the WCG Instutitional Review Board. It has been registered at clinicaltrials.gov. This study will inform the strategy for treatment initiation with buprenorphine among diverse ED settings and will provide ongoing evidence to support the safety and efficacy of initiating treatment for OUD in the ED.
Related protocols: CTN-0145
Purpose: Emergency Departments (ED) are important settings for initiating care following a non-fatal opioid overdose (NFOO). While ED-based interventions, including peer-led recovery support and initiation of medications for opioid use disorder (MOUD), are promising methods for reducing subsequent overdoses and mortality, randomized trials of ED-based overdose prevention or treatment- linkage interventions demonstrate that a substantial proportion of patients decline participation. The current secondary analysis is designed to characterize individuals who declined to participate in one such study.
Methods: Data were used from the Peer Intervention to Link Overdose Survivors to Treatment (PILOT) trial (CTN-0107), which was a multi-site study conducted in three US-based EDs that randomized participants to a 6-month peer-led overdose prevention intervention or treatment as usual in the ED. Demographics and clinical characteristics of those enrolled in PILOT (n = 150) were compared to those who declined to participate but completed a screening exit survey (ScrES; n = 46).
Results: Among those who declined study participation, 76% had experienced a prior overdose preceding the current overdose that brought them into the ED (58.7% within the past 72 h), 56.5% were not currently engaged in substance use treatment and among those, 65.4% expressed a desire for treatment. Odds of declining study participation decreased with age by 6% per year (OR = 0.94, 95% CI: 0.9, 0.99); those with any college experience had odds of declining at 3 times greater than those without a high school diploma (OR = 3.4, 95% CI: 1.2, 10.1). Those without health insurance had odds of declining nearly 3 times those with insurance (OR = 2.9, 95% CI: 1.2, 7.0). Frequently cited reasons for declining were a desire to leave the ED or feeling unwell (39.1%), lack of interest in research (30.4%) and a belief the intervention would not be helpful (17.4%).
Conclusions: Results from this analysis characterize ED patients declining to participate in peer-led overdose prevention research with the goals of enhancing future recruitment strategies and enrolling more representative samples to reduce subsequent overdoses. Future work is needed to determine how to better engage priority populations at critical touch points, while ensuring that interventions are flexible, patient-centered, and potentially offer remote access.
Related protocols: CTN-0107
Given the disproportionate impact of substance use on individuals, families, and communities from populations underrepresented in clinical trials, increasing their enrollment in treatment research is critical for ensuring that the findings inform policies and programs that are inclusive of all communities, thereby advancing health equity. However, since underrepresented groups continue to be underenrolled in clinical trials testing the efficacy and effectiveness of psychosocial treatments for substance use disorder, substance use researchers are still grappling with this challenge.
In this commentary, we describe rigorous methodological approaches, such as integrative data analysis (IDA) and related methods (e.g., moderated nonlinear factor analysis and propensity score weighting), that can help address the challenges posed by the underrepresentation of certain populations. By combining individual-level data from multiple studies into a pooled dataset, these methods increase sample size and statistical power while addressing covariate imbalance across treatment groups. We describe how we employed these methods to address the aims of our recently completed secondary data analysis project conducted within the National Drug Abuse Treatment Clinical Trial Network (CTN-0125; Integrative Data Analysis of CTN Studies to Examine the Impact of Psychosocial Treatments for Black People Who Use Cocaine and/or Opioids). Our study used these methods to pool and analyze data from nine completed CTN trials to assess the comparative effectiveness of psychosocial treatments for Black adults who use cocaine and/or opioids, a group underrepresented in registered trials of the NIDA. We illustrate the application of these methodological approaches in CTN-0125 and demonstrate how they complement each other to address unique analytic challenges. We describe how we addressed data harmonization challenges due to variations in data formats and inconsistencies or gaps in the supportive documentation available on the NIDA Data Share website. We conclude with recommendations for the research field on how to further address sample size and data integration challenges.
Related protocols: CTN-0125
Background: Craving is a core clinical feature of cannabis use disorder (CUD) and a predictor of treatment outcomes, yet its temporal course during treatment is not well characterized. This study aimed to identify latent classes of cannabis craving trajectories among adults with CUD and examine associated baseline predictors and cannabis use outcomes.
Methods: This was a secondary analysis of the National Drug Abuse Treatment Clinical Trials Network’s CTN-0053 trial, a 12-week, multisite randomized controlled trial of N-acetylcysteine versus placebo for adults with CUD (N = 302). Cannabis craving was measured using the Marijuana Craving Questionnaire–Short Form at six treatment timepoints (weeks 1–5, 9 and 12) and one 5-week post-treatment follow-up (week 17). Urine cannabinoid tests were conducted twice weekly throughout treatment and follow-up. Latent class growth analysis identified craving trajectories. The present study aimed to identify latent classes of cannabis craving over 12 weeks of treatment and examine baseline predictors of class membership.
Results: A four-class solution provided the best fit: low craving (41%), moderate-decreasing craving (38%), moderate-stable craving (11%), and high craving (10%). Participants in higher craving classes exhibited greater baseline anxiety, depression, and obsessive-compulsive symptoms related to cannabis use. The high craving class had the greatest proportion of cannabis positive urine tests (96%) and the lowest urine test completion rate.
Conclusions: Craving follows heterogeneous trajectories during CUD treatment and is associated with co-occurring mental health symptoms and poorer outcomes. Dynamic craving assessment may support personalized treatment and strategies to prevent return to use.
Related protocols: CTN-0053
Introduction: Moral injury is the psychological distress resulting from actions, or the lack thereof, which violate one’s moral or ethical code. There is a notable gap in literature exploring moral injury among substance use disorder (SUD) treatment and community service providers. Despite the lack of literature describing moral injury among the SUD workforce, moral injury was discussed extensively during meetings of the Community Representative Council (CIRCL) of the National Drug Abuse Treatment Clinical Trials Network (CTN), which engages community members within the CTN Nodes to understand perspectives of people with lived/living experience and those providing substance use services.
Methods: In response to this consistently raised topic, this commentary reviews the literature on moral injury related to the SUD workforce, as well as the perspectives of CIRCL members on the unique and persistent challenges faced by SUD treatment and community services providers.
Results: Members of CIRCL in the SUD treatment and community provider workforce consistently described experiencing morally injurious events, including acts of commission and omission, bearing witness, and observing betrayal from those in power. While some experiences are akin to those experienced by providers in other healthcare settings, some were unique to front-line SUD treatment and community services providers. These experiences caused intense experiences of guilt, isolation, and hopelessness, sometimes contributing to turnover.
Conclusions: Addressing moral injury among the SUD provider workforce may require unique mitigation and prevention strategies, potentially involving structural changes at the organizational, social, and policy levels that support the SUD treatment and community service workforce, ultimately improving not just the wellbeing of providers and patients, but the wellbeing of our communities.
Authentic community engagement requires partnership with those who share similar situations, concerns, or challenges. Community engagement in research can promote equitable representation, help inform important research questions and deliverables, and increase the likelihood of developing relevant and appropriate interventions that will be implemented and sustained. Established in 1999, the National Drug Abuse Treatment Clinical Trials Network (CTN) is a cooperative agreement within the National Institute on Drug Abuse (NIDA) and functions as a nationwide consortium of research scientists, treatment providers and other community members collaborating to improve care for substance use in communities across the US. The CTN is committed to community-engaged research. Developed in 2023, the CTN Community Representative Council (CIRCL) formed as a natural progression of this commitment, designed to systematically identify front line challenges warranting research and to recognize emerging community-based innovations – forms of “practice-based evidence” developed in response to real-world needs. CTN Nodes (regional hubs) nominated community members, many of whom are people with lived experience (PWLE) of substance use to serve as Council representatives to enhance the identification, communication, and dissemination of the needs and experiences of individuals served by CTN research across the US. This commentary provides an overview of CIRCL’s conceptualization and creation, operation, and impacts on CTN communities in its first year.

Objectives: To identify and value resources required to implement and sustain the Massachusetts model of office-based addiction treatment (MA Model) in the Primary Care Opioid Use Disorders Treatment trial (NCT03407638) using a nurse care manager (NCM) to support medication for opioid use disorder in primary care settings.
Study design: A site-specific microcosting analysis was conducted via activity-based costing. Guided by a structured costing instrument, we conducted semistructured interviews with relevant personnel and assigned nationally representative costs.
Methods: Data came from 6 health care systems. Costs were categorized as fixed start-up, time dependent, or variable and estimated as annual per-clinic and per-patient costs for implementation and sustainment phases.
Results: Mean implementation cost (ie, year 1 fixed start-up, time-dependent, and variable) was $238,888 per clinic ($3185 per patient); each subsequent year cost $229,676 ($3062 per patient), assuming 75 patients per month and 29% new patient case mix. Mean onetime fixed start-up costs were $9212 per clinic and included supplies and training. Time-dependent costs were $70,446 per clinic and included rent and meetings. Variable costs were $159,229 per clinic and included NCMs’ and prescribers’ clinical duties. On average, NCMs spent 1967.6 hours on MA Model-related work per year (26.2 hours per patient). In sensitivity analyses, costs varied drastically with patient caseload, provider mix, and new patient case mix.
Conclusions: Fixed start-up and time-dependent costs were minimal. Variable costs were 66.7% of implementation costs and 69.3% of costs annually afterward. The primary cost driver was NCM time conducting MA Model-related work. The additional value of the model will depend on associated downstream outcomes. These results may be helpful to health care systems considering implementing the MA Model.
Related protocols: CTN-0074
This is the primary outcomes article for CTN-0080-A-2. Introduction: Racial and ethnic inequities persist in medication treatment initiation and adherence for pregnant and postpartum people with opioid use disorder (OUD). Our objective was to understand the experiences of “positive outliers,” specifically pregnant and postpartum people of color with OUD who utilized medication treatment and engaged in a randomized clinical trial for buprenorphine despite historical, cultural, and structural barriers.
Methods: We conducted two sets of semi-structured qualitative interviews. First, trained peers with lived expertise as mothers in recovery interviewed individuals who identified with a non-white race and/or ethnicity and enrolled in the Medication Treatment for OUD in Expectant Mothers (MOMs) trial (NCT03918850). Second, we interviewed principal investigators, clinicians, and research coordinators from the 13 MOMs trial sites. We used an inductive thematic approach informed by the Social Ecological Model of Racism and Anti-Racism. Transcripts were double-coded and reviewed until consensus was reached. Preliminary findings from participant and staff interviews were merged and triangulated with peers to inform theme development.
Results: We completed 17 interviews with MOMs trial participants from 7 sites. Participants identified as Hispanic (29%), Black non-Hispanic (24%), multi-racial Hispanic (18%), multi-racial non-Hispanic (18%), and American Indian, Native Hawaiian, or Pacific Islander (12%). Thirty-two interviews with trial staff were also completed. Three themes emerged: (1) Although some participants expected racist treatment and research exploitation, all participants interviewed reported non-discriminatory, non-judgmental care within the MOMs trial; (2) Compassionate care, frequent, personalized, and integrated encounters, and emotional support helped counteract prior stigmatizing and discriminatory health care interactions, enabling participants of color to feel particularly supported, trusted, and empowered during the MOMs trial; and (3) Despite pervasive cultural stigma around addiction and concerns about taking an investigational drug while pregnant, participants expressed that pregnancy status, care team trust, and transparent communication with MOMs trial staff encouraged medication utilization and adherence.
Conclusion: Facilitators of successful engagement in the MOMs trial and retention in medication treatment among pregnant and postpartum people of color with OUD included non-judgmental care, sustained trust, and frequent contact. Key perinatal OUD clinical interventions and trial improvements include personalized communication and scheduling flexibility to promote engagement of marginalized populations.
Related protocols: CTN-0080-A-2